View this video about the role of GFAP and UCH-LQ in assessing mTBI.
Global point of care
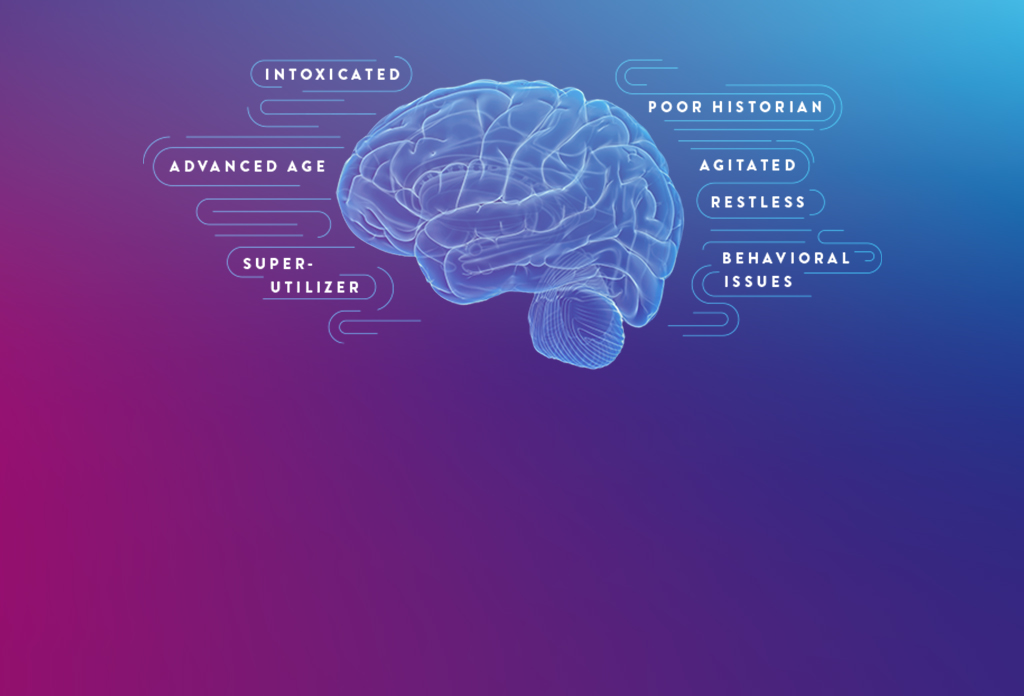


Millions of patients undergo emergency department (ED) evaluation for mTBI each year. Neurocognitive assessments, such as the Glasgow Coma Scale (GCS) and clinical decision rules (CDRs), are subjective and can be difficult to perform with certain patients, such as those who are intoxicated or have an altered mental health status.¹
As a result, you may decide to order a CT, despite having low clinical suspicion of intracranial bleeding. In fact, while an estimated 82% of patients with TBI undergo CT, more than 90% show no evidence of traumatic abnormality.² What’s more, some patients may insist on a CT even though you deem it unwarranted.
The i-STAT TBI Plasma test may be the solution to provide objective data without time-consuming and often avoidable head CTs for mTBI.
In addition to the limitations of clinical decision rules (CDRs) in evaluating some patients with suspected mTBI, patients may present in a way that complicates the logistics of performing a CT scan and may even require sedation, which can further complicate and delay evaluation.


GFAP and UCH-L1 are well validated, complementary, brain-specific biomarkers released into the bloodstream from two different cell types following traumatic brain injury.

View this video about the role of GFAP and UCH-LQ in assessing mTBI.
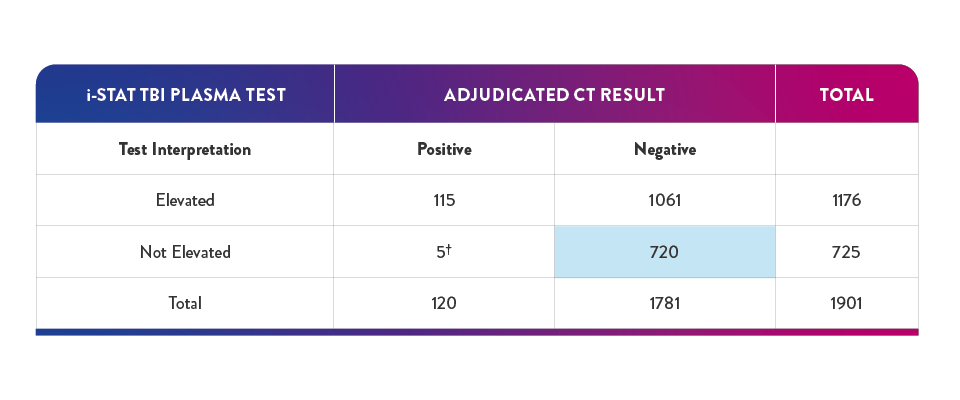
40.4% of negative results in the pivotal study had a true negative result† on the i-STAT TBI Plasma test—suggesting a potential reduction in unnecessary CT of up to 40%6,16
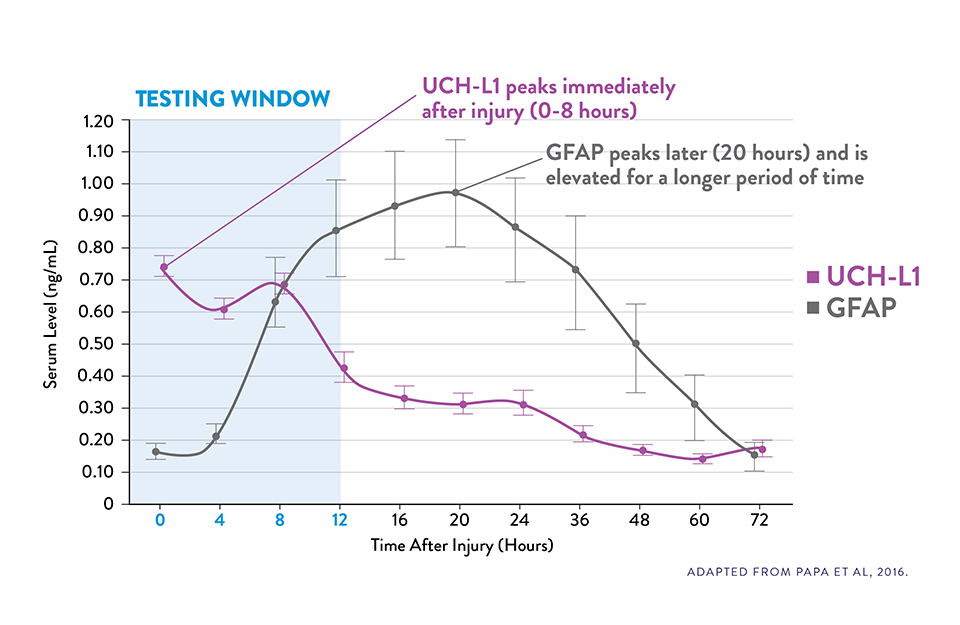
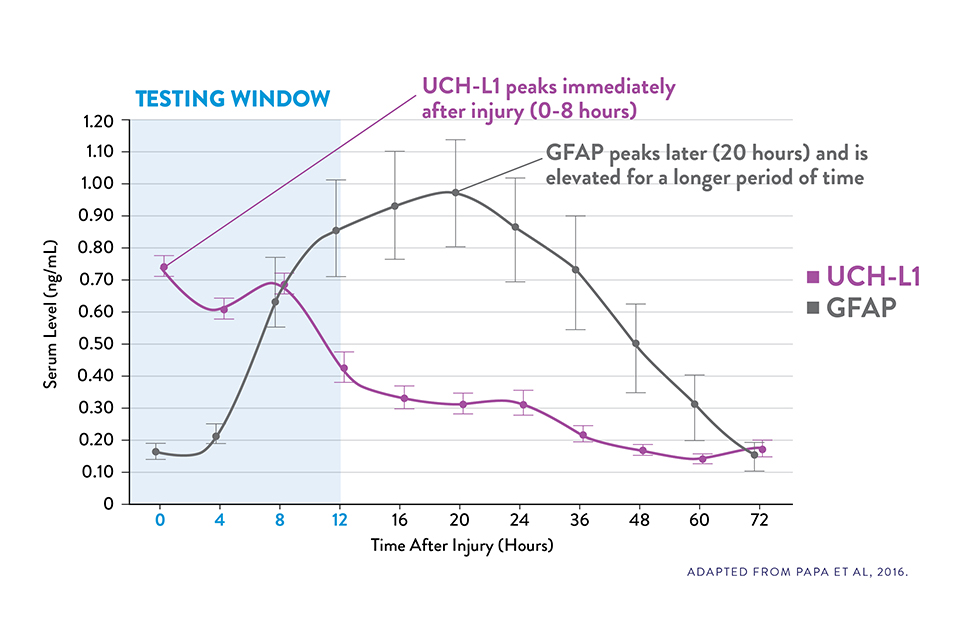
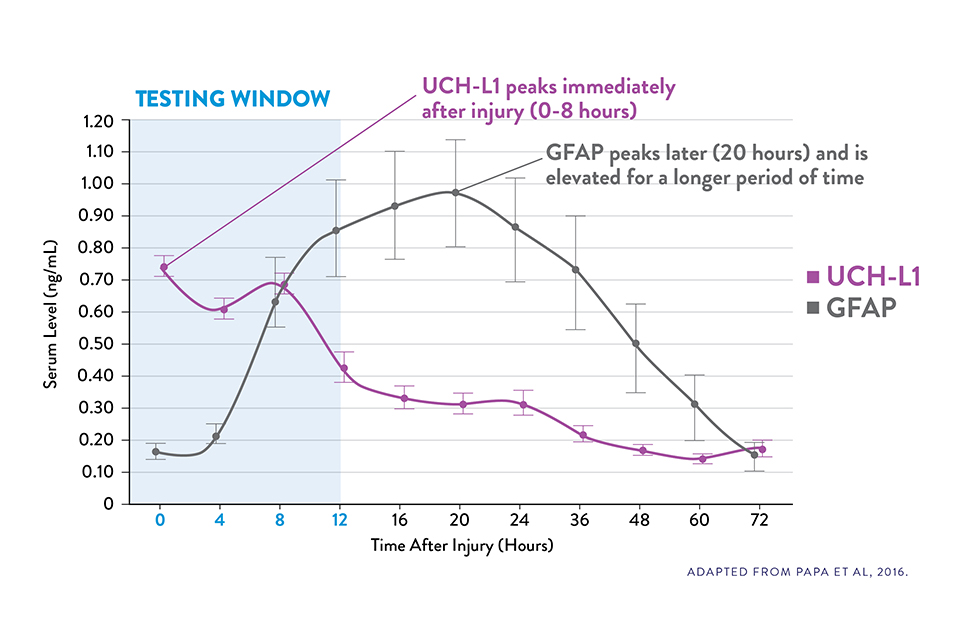
Serum UCH-L1 levels peak 0 to 8 hours post injury and steadily decrease over 48 hours while GFAP peaks at 20 hours and declines slowly 72 hours after brain injury.15
The i-STAT TBI Plasma test measures levels of both biomarkers during the optimal 12-hour period following injury.6‡
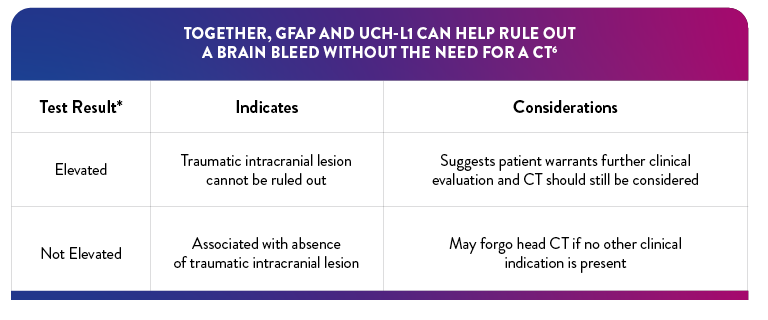
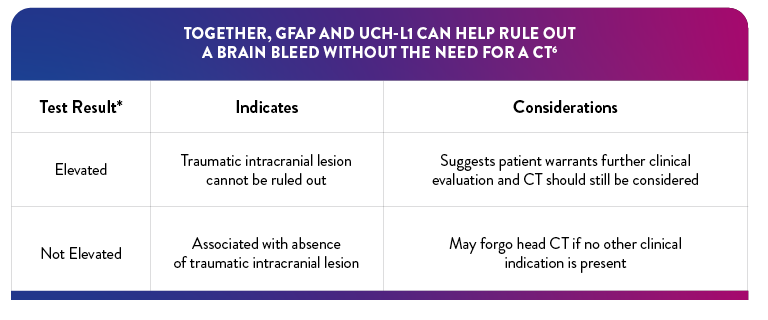
*If either biomarker is above the specified threshold, the result is "elevated"
†True negative result corresponds to clinical specificity
‡The i-STAT TBI Plasma test is to be used with plasma prepared from EDTA-anticoagulated specimens in clinical laboratory settings by a healthcare professional. It is not intended for point-of-care use.
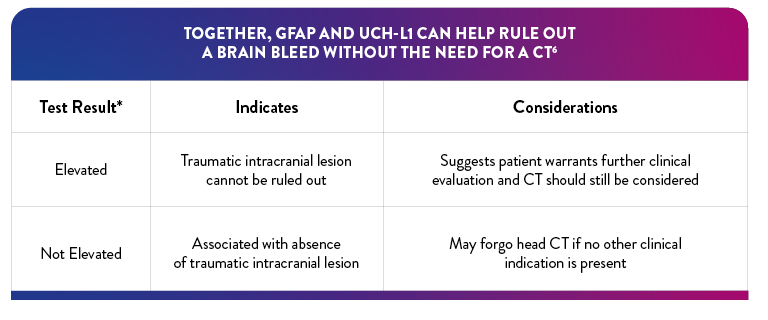
The i-STAT TBI Plasma test combines two brain-specific and complementary biomarkers, GFAP and UCH-L1, in a single, multiplex test designed to optimize sensitivity and negative predictive value (NPV) to help determine the need for CT.
Visit these product pages for details.

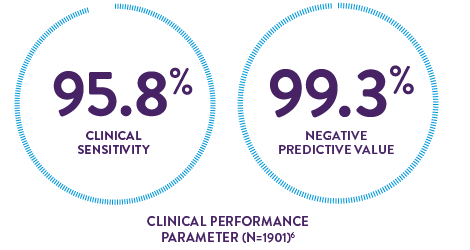
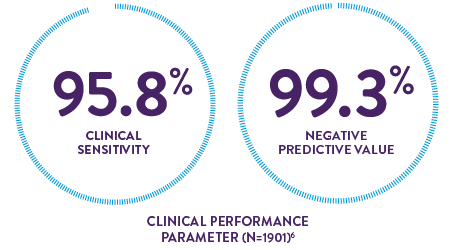
The high clinical sensitivity and NPV of the i-STAT TBI Plasma test provide confidence in aiding decisions for the safe discharge of patients without performing CT
15-minute instrument time6* may provide shorter wait times and timely discharge
*After obtaining plasma sample.
This test is to be used with plasma in clinical laboratory settings by a healthcare professional.
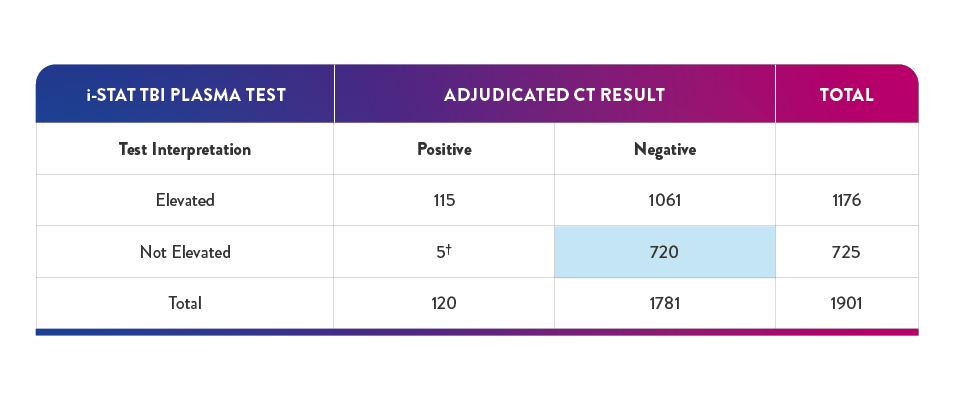
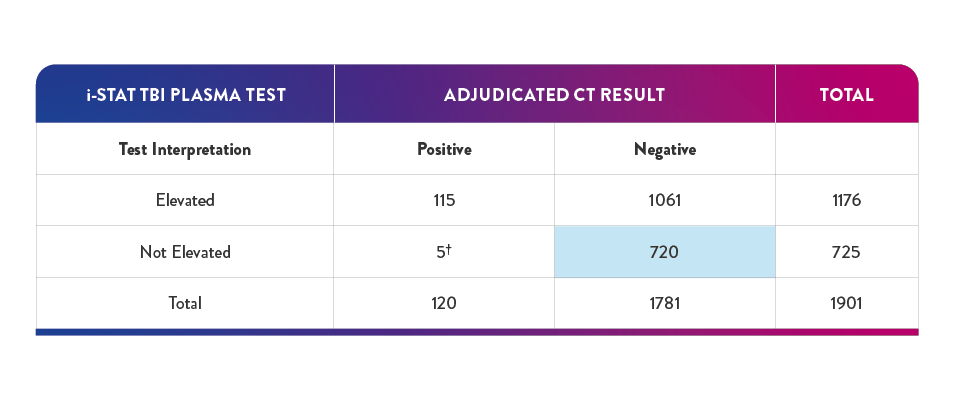
"Elevated" Test interpretation suggests further evaluation by CT should be considered6
"Not Elevated" Test interpretation is associated with the absence of acute traumatic intracranial lesions on CT6
40.4% of negative results in the pivotal study had a true negative result on the i-STAT TBI Plasma test -suggesting a potential reduction in unnecessary CT of up to 40%6,16
*In the study, 5 participants with "not elevated" test findings and a "positive" CT finding, no neurosurgical intervention was required
†True negative result corresponds to clinical specificity
Offers a new adjunct assessment tool in mTBI evaluation, especially when there is clinical uncertainty
Potential to improve ED workflow and optimize resource utilization by reducing avoidable CT and improving patient throughput

1. Centers for Disease Control and Prevention. Get the facts about TBI. May 12, 2021. Accessed January 18, 2023. https://www.cdc.gov/traumaticbraininjury/get_the_facts.htm
2. Korley FK, Kelen GD, Jones CM, Diaz-Arrastia R. Emergency department evaluation of traumatic brain injury in the United States, 2009-2010. J Head Trauma Rehabil. 2016;31(6):379-387.
3. US Food and Drug Administration. What are the radiation risks from CT? Updated December 5, 2017. Accessed February 9, 2023.
https://www.fda.gov/radiation-emitting-products/medical-x-ray-imaging/what-are-radiation-risks-ct.
4. Zetterberg H, Blennow K. Fluid biomarkers for mild traumatic brain injury and related conditions. Nat Rev Neurol. 2016;12(10):563-574.
5. Chodobski A, Zink BJ, Symydynger-Chodobska J. Blood-brain barrier pathophysiology in traumatic brain injury. Trans Stroke Res. 2011;2(4):492-516.
6. i-STAT TBI Plasma Cartridge. Instructions for use. Abbott Point of Care Inc. Abbott Park, IL; 2021.
7. Metting Z, Wilezak N, Rodiger LA, et al. GFAP and S100B in the acute phase of mild traumatic brain injury. Neurology. 2012;78(18):1428-1433.
8. Papa L, Lewis LM, Falk JL, et al. Elevated levels of serum glial fibrillary acidic protein breakdown products in mild and moderate traumatic brain injury are associated with intracranial lesions and neurosurgical intervention. Ann Emerg Med. 2012;59(6):471-483.
9. Jones A, Jarvis P. Review of the potential use of blood neuro-biomarkers in the diagnosis of mild traumatic brain injury. Clin Exp Emerg Med. 2017;4(3):121-127.
10. Schulte S, Podlog LW, Hamson-Utley JJ, et al. A systematic review of the biomarker S100B: implications for sport-related concussion management. J Athl Train. 2014;49(6):830-850.
11. Steiner J, Bernstein H-G, Bielau H, et al. Evidence for a wide extra-astrocytic distribution of S100B in human brain. BMC Neurosci. 2007;8:2.
12. Pelinka LE, Kroepfl A, Schmidhammer R, et al. Glial fibrillary acidic protein in serum after traumatic brain injury and multiple trauma. J Trauma. 2004;57(5):1006-1012.
13. Diaz-Arrastia R, Wang KKW, Papa L, et al. Acute biomarkers of traumatic brain injury: relationship between plasma levels of ubiquitin C-terminal hydrolase-Li and glial fibrillary acidic protein. J Neurotrauma. 2014;31(1):19-25.
14. Papa L, Lewis LM, Silvestri S, et al. Serum levels of ubiquitin C-terminal hydrolase (UCH-L1) distinguish mild traumatic brain injury (TBI) from trauma controls and are elevated in mild and moderate TBI patients with intracranial lesions and neurosurgical intervention. J Trauma Acute Care Surg. 2012;72(5):1335-1344.
15. Papa L, Brophy GM, Welch RD, et al. Time course and diagnostic accuracy of glial and neuronal blood biomarkers GFAP and UCH-L1 in a large cohort of trauma patients with and without mild traumatic brain injury. JAMA Neurol. 2016;73(5):551-560.
16. Data on file. Abbott Point of Care Inc.
In addition to the limitations of clinical decision rules (CDRs) in evaluating some patients with suspected mTBI, patients may present in a way that complicates the logistics of performing a CT scan and may even require sedation, which can further complicate and delay evaluation.

GFAP and UCH-L1 are well validated, complementary, brain-specific biomarkers released into the bloodstream from two different cell types following traumatic brain injury.

View this video about the role of GFAP and UCH-LQ in assessing mTBI.

Explore the science behind the evaluation of traumatic brain injury.
40.4% of negative results in the pivotal study had a true negative result† on the i-STAT TBI Plasma test—suggesting a potential reduction in unnecessary CT of up to 40%6,16
Serum UCH-L1 levels peak 0 to 8 hours post injury and steadily decrease over 48 hours while GFAP peaks at 20 hours and declines slowly 72 hours after brain injury.15
The i-STAT TBI Plasma test measures levels of both biomarkers during the optimal 12-hour period following injury.6‡
*If either biomarker is above the specified threshold, the result is "elevated"
†True negative result corresponds to clinical specificity
‡The i-STAT TBI Plasma test is to be used with plasma prepared from EDTA-anticoagulated specimens in clinical laboratory settings by a healthcare professional. It is not intended for point-of-care use.
The i-STAT TBI Plasma test combines two brain-specific and complementary biomarkers, GFAP and UCH-L1, in a single, multiplex test designed to optimize sensitivity and negative predictive value (NPV) to help determine the need for CT.
Visit these product pages for details.
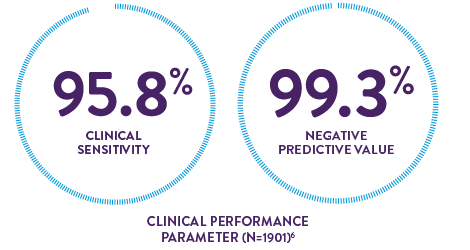
The high clinical sensitivity and NPV of the i-STAT TBI Plasma test provide confidence in aiding decisions for the safe discharge of patients without performing CT
15-minute instrument time6* may provide shorter wait times and timely discharge
*After obtaining plasma sample.
This test is to be used with plasma in clinical laboratory settings by a healthcare professional.
"Elevated" Test interpretation suggests further evaluation by CT should be considered6
"Not Elevated" Test interpretation is associated with the absence of acute traumatic intracranial lesions on CT6
40.4% of negative results in the pivotal study had a true negative result on the i-STAT TBI Plasma test -suggesting a potential reduction in unnecessary CT of up to 40%6,16
†In the study, 5 participants with "not elevated" test findings and a "positive" CT finding, no nuerosurgical intervention was required
‡True negative result corresponds to clinical specificity
Offers a new adjunct assessment tool in mTBI evaluation, especially when there is clinical uncertainty
Potential to improve ED workflow and optimize resource utilization by reducing avoidable CT and improving patient throughput
1. Centers for Disease Control and Prevention. Get the facts about TBI. May 12, 2021. Accessed January 18, 2023. https://www.cdc.gov/traumaticbraininjury/get_the_facts.htm
2. Korley FK, Kelen GD, Jones CM, Diaz-Arrastia R. Emergency department evaluation of traumatic brain injury in the United States, 2009-2010. J Head Trauma Rehabil. 2016;31(6):379-387.
3. US Food and Drug Administration. What are the radiation risks from CT? Updated December 5, 2017. Accessed February 9, 2023.
https://www.fda.gov/radiation-emitting-products/medical-x-ray-imaging/what-are-radiation-risks-ct.
4. Zetterberg H, Blennow K. Fluid biomarkers for mild traumatic brain injury and related conditions. Nat Rev Neurol. 2016;12(10):563-574.
5. Chodobski A, Zink BJ, Symydynger-Chodobska J. Blood-brain barrier pathophysiology in traumatic brain injury. Trans Stroke Res. 2011;2(4):492-516.
6. i-STAT TBI Plasma Cartridge. Instructions for use. Abbott Point of Care Inc. Abbott Park, IL; 2021.
7. Metting Z, Wilezak N, Rodiger LA, et al. GFAP and S100B in the acute phase of mild traumatic brain injury. Neurology. 2012;78(18):1428-1433.
8. Papa L, Lewis LM, Falk JL, et al. Elevated levels of serum glial fibrillary acidic protein breakdown products in mild and moderate traumatic brain injury are associated with intracranial lesions and neurosurgical intervention. Ann Emerg Med. 2012;59(6):471-483.
9. Jones A, Jarvis P. Review of the potential use of blood neuro-biomarkers in the diagnosis of mild traumatic brain injury. Clin Exp Emerg Med. 2017;4(3):121-127.
10. Schulte S, Podlog LW, Hamson-Utley JJ, et al. A systematic review of the biomarker S100B: implications for sport-related concussion management. J Athl Train. 2014;49(6):830-850.
11. Steiner J, Bernstein H-G, Bielau H, et al. Evidence for a wide extra-astrocytic distribution of S100B in human brain. BMC Neurosci. 2007;8:2.
12. Pelinka LE, Kroepfl A, Schmidhammer R, et al. Glial fibrillary acidic protein in serum after traumatic brain injury and multiple trauma. J Trauma. 2004;57(5):1006-1012.
13. Diaz-Arrastia R, Wang KKW, Papa L, et al. Acute biomarkers of traumatic brain injury: relationship between plasma levels of ubiquitin C-terminal hydrolase-Li and glial fibrillary acidic protein. J Neurotrauma. 2014;31(1):19-25.
14. Papa L, Lewis LM, Silvestri S, et al. Serum levels of ubiquitin C-terminal hydrolase (UCH-L1) distinguish mild traumatic brain injury (TBI) from trauma controls and are elevated in mild and moderate TBI patients with intracranial lesions and neurosurgical intervention. J Trauma Acute Care Surg. 2012;72(5):1335-1344.
15. Papa L, Brophy GM, Welch RD, et al. Time course and diagnostic accuracy of glial and neuronal blood biomarkers GFAP and UCH-L1 in a large cohort of trauma patients with and without mild traumatic brain injury. JAMA Neurol. 2016;73(5):551-560.
16. Data on file. Abbott Point of Care Inc.
A leader in rapid point-of-care diagnostics.
©2024 Abbott. All rights reserved. Unless otherwise specified, all product and service names appearing in this Internet site are trademarks owned by or licensed to Abbott, its subsidiaries or affiliates. No use of any Abbott trademark, trade name, or trade dress in this site may be made without the prior written authorization of Abbott, except to identify the product or services of the company.
This website is governed by applicable U.S. laws and governmental regulations. The products and information contained herewith may not be accessible in all countries, and Abbott takes no responsibility for such information which may not comply with local country legal process, regulation, registration and usage.
Your use of this website and the information contained herein is subject to our Website Terms and Conditions and Privacy Policy: US Citizens | Non-US Citizens. Photos displayed are for illustrative purposes only. Any person depicted in such photographs is a model. GDPR Statement
Not all products are available in all regions. Check with your local representative for availability in specific markets. For in vitro diagnostic use only. For i-STAT test cartridge information and intended use, refer to individual product pages or the cartridge information (CTI/IFU) in the i-STAT Support area.
Abbott - A Leader in Rapid Point-of-Care Diagnostics.
